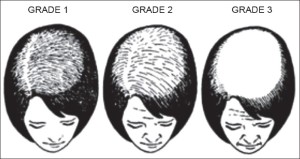
It’s been a little while since I’ve done a blog post. The last blog post was on Female Pattern Hair Loss, a very common and distressing entity. Though the the true cause of FPHL has not been completely determined, it certainly has more medical (non-surgical) treatment options than Male Pattern Hair Loss.
Medical Management of Female Pattern Hair Loss
The medical management of FPHL can be categorised into two types: Topical and Oral.
Topical Treatment of Female Pattern Hair Loss
Topical Minoxidil (Rogaine)
Like Male Pattern Hair Loss, FPHL is treated with the agent Minoxidil. The dose recommended for women is the 2% solution used twice daily or the 5% foam (available only in the brand Rogaine) once daily. To be honest, most hair loss experts like to use the 5% solution or foam twice a day as it just seems to work better. The real problem lies in one of the side effects which is excessive hair growth (hypertrichosis). It is more likely to occur in women and with the 5% concentration used twice daily. To combat this, it is best to decrease the dosing to once a day or once alternate day. Again, like with Male Pattern Hair Loss, it takes 4-6 months with continuous use, to see the benefits.
Oral Treatment of Female Pattern Hair Loss
This medical management of Female Pattern Hair Loss is has many more options for women. Men only have Finasteride (Propecia) available for use, while women typically have four major agents available. Most of these agents are anti-androgen or anti-male hormone, HOWEVER, most women with Female Pattern Hair Loss have been found to not have excessive male hormones. The interest thing however, is that they still respond to the use of these agents. Why this is so, is still being determined scientifically.
Finasteride (Proscar/Propecia)
Finasteride is also used for Female Pattern Hair Loss. This agent is a 5 alpha reductase antagonist. This therefore blocks the formation of dihydrotesterone from testosterone, stopping the more potent androgen from acting on the hair follicle. The optimal effect is at a much higher dose than what is used in men. Again, like with men, it takes about 4 months to see the benefit.
It is not recommended in women who plan to get pregnant. Persons who are in that stage of their life are advised strongly to not get pregnant whilst on the drug as because it is an anti- male hormone drug, it potentially could affect male foetuses. It however, does not stop someone from getting pregnant. In fact we advise persons to try starting conception at least 1 month after stopping the medication.
Dutasteride (Avodart)
This is another 5 alpha reductase inhibitor. However, it is more potent as an anti-androgen as it acts on two forms of the enzyme that converts testosterone to dihydrotestosterone. It is a newer agent that is use off-label mainly for post-menopausal women as it stays in the body for a much longer time than Finasteride. Again, the time to see a difference is up to 4 months of using the medication continuously.
Spironolactone (Aldactone)
Spironolactone is an anti-hypertensive diuretic aka a “water pill” that promotes loss of Sodium in the urine to help aid in dropping the Blood Pressure. It, at a low dose has been used for this indication in both men and women for more than 50 years. At much higher doses, it has anti-male hormone effects. Again, it takes 4 months to see any difference.
It is used more in women with an underlying cause of Female Pattern Hair Loss such as Polycystic Ovarian Syndrome (PCOS). It can reduce body hair on the chin and chest BUT it increases the growth of hair on the head. It is used more in pre-menopausal women.
This medication is used a lot in the United States where Diane 35 is not available.
Cyproterone acetate (Androcur)
This is another anti-male hormone medication that has been used in pre-menopausal women. It is present in low doses in certain contraceptive pills such as Diane 35 which is found in many countries other than the United States. For effective control of hair loss, Androcur is used because it is at a higher dose. Again, women are advised not to get pregnant whilst taking the medication.
Flutamide
This is another anti-androgen medication that is available in the arsenal of medication for Female Pattern Hair Loss. The problem with this medicaiton is that it can cause severe liver toxicity. Most use this as a last resort.
To get optimal effects, a combination of topical and oral modalities is preferred especially since in women the true nature of the cause of Female Pattern Hair Loss is not known.
Surgical Management
Like with Male Pattern Hair Loss, sufferers of FPHL can also benefit from hair transplantation. However, women can be poorer candidates than men because their hair loss tends to cover a much larger area from very early. It is quite a successful operation as more than 95% of the transplanted hairs will grow and stay. The main problem is that the original hairs surrounding the transplanted hairs are still being affected by Female Pattern Hair Loss. These hairs will have to be addressed using some sort of medical management or the person will have to end up doing more than one hair transplant in their lifetime. Hopefully hair cloning will be successful and will be available in the future.
Treatment of Female Pattern Hair Loss can be quite tricky, however, the results can be so life changing for women who suffer from this condition.